Representational Structures in Psychopathology [A version of this paper was presented on June 9, 1990, at the Annual Meeting of the Rapaport-Klein Study Group. This is the first part of a two-part presentation. A version of the second part, co-authored by S.J. Blatt and R.B. Blass and titled "Interpersonal Relatedness and Self-Definition: Two Basic Dimensions in Personality Development and Psychopathology", appeared in the book edited by G.G. Noam & K.W. Fischer Development and Vulnerabilities in Close Relationships, Hillsdale, NJ: Erlbaum, 1996, chapter 12, pp. 309-338]
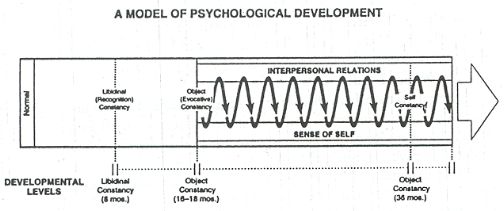
Various forms of adult psychopathology, from schizophrenia to the neuroses (e.g., hysteria), involve fundamental impairments in representational structures or cognitive-affective schema. Concepts from psychoanalysis, cognitive developmental psychology, and attachment theory and research enable us to specify particular nodal points in the development of representational structures, and to consider how disruptions of this developmental process are involved in various forms of psychopathology in adults (Blatt, 1991a). Cognitive-affective schemas are established in interpersonal interactions throughout the life cycle, beginning with the earliest experiences of the infant in the caring relationship with mother. These cognitive-affective schemas are established as the child matures and experiences various developmental demands. When these perturbations are age appropriate and not severe,' the child is able to alter existing cognitive schema to accommodate the experienced perturbations, thereby leading to the development of more comprehensive and mature levels of cognitive schema. This process usually unfolds in a natural, well-defined developmental sequence. When developmental demands are severe, persistent, and overwhelm the child's capacities to accommodate, however, the development of cognitive-affective schemas may be compromised (Blatt, 199la). It is the assumption of this paper that various forms of psychopathology in adults are determined, in large part, by differential impairments of the schemas of the representational world that occur as a consequence of serious disruptions of the relationship between child and caregivers. In the past two decades there has been a remarkable increase in attention directed to the role of interpersonal relations in the psychological development of infants and children as well as adolescents and adults. Much of the research on interpersonal relations with infants and children has directly or indirectly been influenced by the study of the dynamics of attachment and separation first articulated by John Bowlby (1969, 1973) and later enriched by the work of Mary Ainsworth (1969), Mary Main (1985) and Inge Bretherton (1985). Attachment theory emerged from Bowlby's observations of the pervasive disruptive consequences of maternal deprivation in institutionalized children separated from their primary caregiver (usually mother). His observations suggested that: "the young child's hunger for his mother's love and presence is as great as his hunger for food," and that her absence inevitably generates "a powerful sense of loss and anger" (Bowlby, 1969, p. xiii). Based on ethological theory, Bowlby postulated that the infant-caregiver attachment bond is a complex, instinctually guided, behavioral system that has functioned throughout human evolution to protect the infant from danger. Secure attachment in infancy is based on the mothers reliable and sensitive provision of safety and love as well as food and warmth. There are consistent differences, however, in the degree to which infant-mother relationships are characterized by experiences of security. By studying behavioral patterns of attachment and separation between mothers and their infants in the first eighteen months of life, Bowlby, Ainsworth, Main and others distinguished secure attachment from several types of insecure attachment, and demonstrated the impact of these attachment styles on subsequent behavior during later childhood years. Based on repeated transactions with attachment figures, infants form mental representations or cognitive-affective schemas of Self and of others, and develop expectations about interpersonal relations. For example, an infant whose needs are typically met inconsistently and unreliably may develop concepts of the self as being unworthy of attention and as incapable of influencing the behavior of others who are perceived as generally inaccessible, uncaring and unresponsive. Conversely, children whose needs have been addressed in a loving and supportive manner may subsequently regard others as reliable and dependable and themselves as competent and worthy of love. These cognitive-affective schemas include a conception of the behavior of significant caring figures as well as a conception of the self in intimate relationships (Bretherton, 1987; Levy, Blatt & Shaver, in press; Zeanah & Anders, 1987). These "internal working models" of caring experiences (Ainsworth, 1969; Bowlby, 1973) organize and influence subsequent personality development and interpersonal relations throughout the life cycle. Attachment theory consists of two parallel but interrelated dimensions: 1) an interactional or behavioral dimension (Bowlby, 1969), based on ethological theory, concerned with the development and maintenance of particular patterns of behavior that are established in infant-parent interactions and 2) a representational or cognitive dimension, based on cognitive developmental and psychoanalytic theories (Bowlby, 1973, 1980; Main, Kaplan & Cassidy, 1985), concerned with how intimate interpersonal interactions are established (internalized or interiorized) in the mind as "internal working models" of caring experiences and how these schemas influence later emotional states and the capacity to develop and maintain intimate relations with others. The interactional or behavioral dimension of attachment theory is based on the assumption chat attachment is a homeostatic behavioral system chat has survival value by regulating the infants proximity seeking and contact maintaining behavior in the second half of the first year of life (6 to 12 months of age) with a specific individual(s) who provides physical safety and psychological security. Attachment behavior, according to Bowlby (1969, p. 129) is "...any form of behavior that results in a person attaining or retaining proximity to some other differentiated and preferred individual, who is usually conceived as stronger and/or wiser." This attachment system is activated by the onset of the infant's locomotion and assertion of physical separation from mother. Initially this separation process, and the beginning exploration of the environment beyond mother, occurs in the protective proximity of the caregiver (Bretherton, 1987), but eventually mother needs to facilitate the child's explorations beyond this protective structure. Based on the quality of the attachment, and the capacity of the mother and child to tolerate separation and to reestablish relatedness upon reunion, Ainsworth and her colleagues identified three types of infant-mother dyads: a) securely attached in which caretakers provide a secure base which enables the infant co-explore the world beyond the relationship with mother and to actively seek contact and interaction with mother after separation from her, b) insecurely avoidant attachment in which the infant can explore the environment but ignores the caregiver upon return after separation, and c) insecurely anxious-resistant (or preoccupied) attachment in which the infant focuses his/her attention on the caregivers, is reluctant to separate, and is clinging and dependent on reunion. Securely attached infants as preschoolers are cooperative, popular with peers and highly resilient and resourceful (Sroufe, 1983), and at age 6 are relaxed and friendly and converse with their parents in a free-flowing and easy manner (Main & Cassidy, 1988). Insecure avoidant infants as preschoolers appear emotionally insulated, hostile and antisocial (Sroufe, 1983), and later tend to distance themselves from their parents and ignore their parents initiatives in conversation (Main & Cassidy, 1988). Anxious-resistant or preoccupied insecure infants are tense and impulsive as toddlers and passive and helpless in preschool (Sroufe, 1983), and later show a mixture of insecurity and hostile behavior in interaction with their parents (Main & Cassidy, 1988). These three attachment patterns are relatively stable over time (Bretherton, 1985) even into early adolescence (age 11) (Elicker & Sroufe, 1992) and they have cross-generational continuity as indicated by mothers reporting similar caring experiences with their own mothers and by the fact that pregnant women report early childhood caring experiences that are congruent with their subsequent caring behavior with their own infants (Fonagy, Steele, Moran, Steele, & Higgit, 1991; Fonagy, Steele & Steele, 1991; Fraiberg, Adelson, & Shapiro, 1976; Main et al., 1985; Slade & Aber, 1992). These patterns of secure and insecure attachment in adults are also characterized by differences in cognitive processes as observed in the degree of cohesion and consistency of narrative reports by adults about their early life experiences. And these attachment patterns have been observed in multiple cultures (e.g., George & Solomon, 1989; Grossman, Fremmer-Bombik, Rudolph & Grossman, 1985; Main et al., 1985; Ricks, 1985; Zeanah et al., 1991). The representational dimension of attachment theory is based on the assumption that the pattern of caring relationships increasingly become a central cognitive-affective structure of the child through the internalization of early parent-child interactions. During the first 18 months of life, the child establishes mental representations or "internal working models" of attachment relationships - "a set of conscious and unconscious rules for the organization of information relevant to attachment and (or obtaining or limiting access to that information, that is, to information regarding attachment-related experiences, feedings and ideations" (Main et al., 1985, p. 67). The affective (or libidinal) attachment between infant and caretaker established during the first year of life evolves into a capacity for object permanence and evocative constancy during the 5econd year that provides a "secure base" (Ainsworth, 1969; Bowlby, 1988) that enables the child to leave the mother in order to explore more fully the world beyond the primary relationship with her. The nature of the attachment relationship, both thc quality of the affective bond and the child's capacity for evocative constancy, markedly influence the way the child deals with this separation. Thus, in addition to noting behavioral continuities across the life cycle, from infancy to adulthood, attachment theory and research posit an important theoretical construct - the internal working model, or cognitive-affective schema, that is established in the experiences of secure and insecure attachment. These cognitive-affective schemas provide templates that maintain the continuity of interpersonal behavior beyond infancy. Attachment theorists have become increasingly interested in understanding more precisely the nature of these cognitive schemas of the representational world as they extended their investigations of interactive behavioral patterns to the ways in which early attachment relationships are subjectively experienced and internally constructed. As noted by Main, Kaplan & Cassidy (1985), the internal working model of attachment established by the end of the first year of life functions as a "template of previously unrecognized strength" (p. 94) which is "related not only to individual patterns in nonverbal behavior, but also to patterns of language and structures of mind" (p. 67). As Bowlby (1988, p. 130) noted 'The working models a child builds of his mother and her ways of communicating and behaving towards him, and a comparable model of his father, together with the complementary models of himself in interactions with each, are being built by a child during the first few years of his life and, it is postulated, soon become established as influential cognitive structures." The patterns of secure, insecure avoidant, and insecure preoccupied attachment establish fundamental cognitive-affective schemas that not only influence behavior in childhood, but also form the basis for normal and deviant behavior in adolescence and adulthood. The cognitive-affective schema or the "internal working model" identified in attachment research is consistent with the research and theoretical formulations o( developmental psychoanalysts, especially object relations theorists, who consider mental representations as pivotal psychological structures in personality development. The concepts of internalization and the differentiation and integration of self and object representations described by psychoanalytic investigators elucidate further the cognitive or representational dimension of the attachment process. The study of mental representations in psychoanalytic object relations is based primarily on the study of psychopathology, especially in adults, whereas the investigation of internal working models in attachment theory derives predominately from the study of the behavior of normal infants and their mothers. Comparisons between attachment and object relations theories have thus far been primarily theoretical (Blatt & Blass, 1991; Lyons-Ruth, 1991; Silverman, 1991; Patterson & Moran, 1988; Zelnick & Buchholtz, 1990), but an integration of concepts from object relations and attachment theories offers the possibility of understanding more fully the complex relationships among interpersonal, affective and cognitive dimensions in both normal and pathological psychological development through- out the life cycle (Diamond & Blatt, 1994). The concept of the internal working model of attachment theory is similar to psychoanalytic concepts of mental representation such as Sandler and Rosenblatt's (1962) representational world as the internal drama in which the individual establishes representations of self and others in multiple roles, and Kernberg's (1993) units of self-object-affect that provide the basis for the formation of self and object representation. Psychoanalytic theorists strc5s the internalization of early interactions with caregivers and how this process results in the formation of representations of self and others, and of their actual and potential relationships (Blatt, 1974; Blatt, Wild and Ritzler, 1975; Kernberg, 1976; Kohut, 1971; Mahler et al., 1975). [Footnote 1: This interest in representational structures that evolve from the internalization of affect-laden caring interactions is an expression of a shift in interests in psychoanalysis from a one person psychology focused on the biological balance between the intensity o(drives and the thresholds of defenses. to a two person psychology focu5cd on the quality of early fundamental caring experiences. The shift to object relations theory within psychoanalysis is consistent with, and in part influenced by, psychoanalytically informed research in infant development (e.g., Emde, 1983; Lichtenberg, 1985: Stern, 1985). The concept of mental representations or internal working model (IWM) of caring relationships, for example, is consistent with Stern's (1985) formulation of the "Representations of Interactions that have been Generalized" (RIGS). Repeated experiences of self and other, organized around particular affects associated with a significant other (e.g., mother, father) and invariant attributes of that interaction (Schank & Abelson, 1977; Stern, 1985), result in the representation of attributes of the self and the other and the affects and actions that connect self and other. The emphasis on internal representations in psychoanalysis and attachment theory is also consistent with developments in social cognition (e.g., Abelson, 1981; Brewer & Nakamura, 1984; Cantor, 1981; Fiske & Taylor, 1984; Hastic, 1981; Kelly, 1955; Kihlstrom & Cantor, 1984; Mandler, 1988; Nelson & Grundel, 1981; Rosenberg, 1988; Taylor & Crocker, 1981) and cognitive- information processing (e.g., Anderson, 1983; Blum, 1985; Erdelyi, 1985; Gardner, 1985; Kihlstrom & Cunningharn, 1991; Rumelhart, 1980).] Both attachment and psychoanalytic object relations theorists have increasingly recognized that the infant does not internalize a static image or representation of the self and of the other, or actual attachment related transactions, but the infant internalizes constructions of various dimensions of the affectively charged relationship between self and other that are established around fundamental experiences of gratification and frustration in caring relationships (Behrends & Blatt, 1985; Bretherton, 1987; Kernberg, 1990,1993; Loewald, 1962; Zeanah & Anders, 1987). Both emotional relatedness and moments of separation, or disruptions of relatedness, that inevitably occur in the course of development, contribute in important ways to the child's internalization of working models or mental representations of attachment relationships. The internalization of caring experiences results in the construction of the representation of self and other, bonded together through affective valences experienced in the caring relationships. These cognitive-affective structures or schema are core aspects of normal as well as pathological psychological development. These representations provide a template for processing and organizing information so that new experiences are assimilated into existing mental structures. The content and structure of these mental representations have both conscious and unconscious components that serve as heuristic guides that organize and direct an individual's behavior, particularly in interpersonal relationships (Blatt & Lerner, 1983). The psychoanalytic concept of the internalization of caring experiences leading to the differentiation, articulation and integration of self and object representations, extend and enrich the contributions of attachment theory and the understanding of the implications of patterns of secure and insecure attachment for psychological development. A basic postulate of both attachment theory and psychoanalytic object relations theory is that relationships with primary caregivers result in the development of cognitive-affective schemas that act as heuristic guides for subsequent interpersonal relationships. Consistent, positive, affective experiences between child and attachment figures result in relatively integrated and differentiated internal working models of attachment relationships in which stable attributes of the attachment relationship become elaborated and consolidated. New experiences over succeeding years and developmental periods are integrated into earlier mental representations, resulting in advances over prior stages such as the development of object and self constancy and of symbolic activity more generally. Significant fluctuations, inconsistencies, disruptions and negative experiences in caretaking interactions, however, can lead to less differentiated, integrated, and consolidated representational schemas that are organized with a more limited focus as individuals attempt to establish a sense of security in distorted and maladaptive ways. The internal working mode[ or mental representation of caring experiences established atound 12 to 18 months of age is an essential component of the development of evocative object constancy (Zeanah & Anders, 1987). Evocative constancy is defined in psychoanalytic theory (e.g., Fraiberg, 1969) as the capacity to establish and sustain a representation of the caregiver, independent o( her physical presence and of variations in the infants need states. This psychoanalytic conception of evocative constancy that develops within an attachment relationship is consistent with the definition of evocative constancy in cognitive developmental theory (e.g., Piaget, 1945/1962) as the ability to sustain a sense of the permanence of an object during its absence from the perceptual field. It is important to stress, however, that evocative constancy is only one, albeit a very important, milestone in the development of cognitive-affective schemas. There are other levels of cognitive-affective schema established in psychological development, some of which precede and others that follow the development of evocative constancy. These various levels of cognitive-affective schema, like evocative constancy, have major roles in psychological development. These various levels of cognitive-affective schema provide developmental markers that can be useful in articulating some of the disrupted representational structures inherent in different forms o( psychopathology in adults. The Development of Cognitive-Affective Schemas Cognitive schemas are long-term, enduring psychological structures, modes of processing and organizing information, including affects, that provide templates that guide and direct an individuals interactions in the interpersonal and impersonal world (Blatt, 1974; Blatt & Lerner, 1983,1992; Blatt, Wild & Ritzler, 1975). Cognitive developmental psychologists, such as Piaget and Werner, have studied how the child develops cognitive schemas but primarily of inanimate objects (e.g., a toy) under essentially neutral circumstances. Psychoanalytic developmental theorists and attachment investigators, in contrast, have studied the very same developmental process, but primarily how the child develops cognitive-affective schema of the interpersonal world (concepts of self and others) in states of disequilibrium (e.g., during separation or moments of unrest), especially in caring relationships. Despite basic differences in methodology, these various approaches to the study of the development of cognitive-affective schemas describe essentially the same developmental sequence, but differ to some degree in the specification of the time at which a particular cognitive-affective schema may first appear. The cognitive developmental theorists usually specify that a particular schema occurs somewhat later than do the developmental psychoanalysts. These differences, however, are consistent with the findings (e.g., Bell, 1970) that cognitive-affective structures emerge initially in the intensity of the caring interpersonal relationship and are subsequently extended as generalized schemas that the child also employs to understand the inanimate world. Cognitive-affective schemas emerge first and foremost in the caring relationship and are then stabilized as generalized cognitive structures. Since these various developmental investigators and theorists describe essentially the same developmental sequence for the emergence of cognitive-affective schemas, their findings can be integrated into a consistent theoretical model. Table 1 presents an overview of various levels in the development of cognitive schema. Table 1 Levels of Cognitive Schema: Developmental Levels and Behavioral Indications I. Developmental Level: Boundary Constancy (2-3 months). Behavioral Indication: Smiling response, initiates engagement with others. II. Developmental Level: Recognition (libidinal) Constancy (6-8 months). Behavioral Indication: Stranger anxiety, differentiation among people, libidinal attachment to a specific individual. III. Developmental Level: Evocative Constancy (16-18 months). Behavioral Indication: Sense of object not immediately present in perceptual field. Anticipation of invisible displacement (Piaget), initiate separation from caring agent (Mahler). IV. Developmental Level: Self and Object Constancy (30-36 months). Behavioral Indication: Stable concepts of self and other, as expressed in use of terms such as "mine," "me," and "I" V. Developmental Level: Concrete Operational Thought (5 years). Behavioral Indication: Capacity for coordinating several dimensions simultaneously Capacity for anticipation, transformation, conservation, and reversibility of external manifest features. Triadic configurations and the emergence of a concept of "we." VI. Developmental Level: Formal Operational Thought (11-12 years). Behavioral Indication: Transformation, reversibility and conservation of abstract, inner features, dimensions, and processes such as values and principles. Recognition that one constructions meaning and a sense of reality. Appreciation of personal and cultural relativism. VII. Developmental Level: Self Identity (late adolescence- young adulthood). Behavioral Indication: Synthesis and integration of mature expressions of both individuality and relatedness in a capacity to be intimate with another and to contribute to a collective without losing ones individuality. Emergence of a fuller sense of "we" (e.g., "self-in-relation" [Chodorow, 1978, 1989; Gilligan, 1982; Miller, 1976] or "ensembled individualism" [Sampson, 1985, 1988]). VIII. Developmental Level: Integrity (mature adulthood). Based on an integration of concepts from cognitive developmental psychology, developmental psychoanalytic theory, and attachment theory and research, one can specify several major nodal points in the development of cognitive-affective schemas from infancy through adulthood. The first level can be identified as boundary constancy. The development of this schema, around the age of 2 to 3 months, is indicated behaviorally by the infants intentional smiling response and the infants capacity to initiate engagement with others. The infant's early spontaneous smile to another suggests that the infant has articulated the physical form of a person from the embedding field and is responsive to it. Consistent with experimental studies of visual gaze in infants (e.g., Fantz, 1963, 1966; Fantz & Nevis, 1967) as well as in infra-human species (e.g., Hubel & Wiesel, 1959, 1962), Piaget (1926/1955) and Werner (1948/1957; Werner & Kaplan, 1963) also discuss the child's first cognitive schema as involving the articulation of the fundamental contour or boundary of an object from an embedding context. Later in development, around 6 or 8 months, the infant begins to distinguish among people, develops an intense investment in a few people, and differentiates these particular persons from others. The child responds to mother and/or father in a special way in contrast to strangers. The child has developed a cognitive-affective schema we can call recognition or libidinal constancy (e.g., Fraiberg, 1969) in which the child no longer just articulates the form of an individual from an embedding field, but is now differentially responsive to the familiar and the special. The development of this attachment bond to a particular person or persons, indicates that child has developed a stable and consolidated capacity for recognition. This affective bond and recognition constancy are essential for later development since they provide the base necessary for the development of secure attachment. As discussed by Bowlby, Ainsworth, Bretherton and others, the security of attachment, however, will also be influenced by the way the mother and the child manage separations and other disruptions that naturally occur to interrupt this attachment bond. At about 16 months, a third level of cognitive-affective schema emerges called evocative object constancy - the capacity to retain and recall a conception of an object that is no longer immediately present in the perceptual field. As described in detail in psychoanalytic discussions of the rapprochement phase (e.g., Mahler, Pine & Bergman, 1975) and in attachment theory and research, the child can begin to leave the mother without undue distress because the child can now maintain a sense of the mother in her absence. Piaget (1926/1955) and Werner (1948/1957; Werner & Kaplan, 1963) also discuss the emergence of the child's capacity for evocative constancy in their observations of the development of the child's ability to anticipate invisible displacements of an object. Patterns of secure and in5ecure attachment become apparent around the development of evocative object constancy. As discussed by attachment theorists, the internal working models of caring experiences consist of the mental representation of the self in interaction with others including the availability and consistency of attachment figures and the worthiness of the self as deserving of, and able to, obtain security and comfort (Bowlby, 1969; Kobak & Hazan, 1991). Thus, evocative object constancy not only marks the development of a stable concept of the object, but it also marks the emergence of a stable sense of self. At about the age of 3 years the child begins to develop a consolidated sense of self as separate from and independent of others. The emergence of this self constancy is indicated by the child's increasing ability to use the terms "mine," "me," and "I" with specificity and precision. The child is increasingly able to differentiate between self and others and to be aware of differences in his/her relationship with others. With the development of both object and self constancy, concepts of the self and of others now develop in a reciprocal or dialectic interaction, such that further differentiation affects the representation of both self and others, as well as thc relationship between self and others. The emerging sense of self facilitates the development of more mature levels of interpersonal relatedness and, conversely, new types of interpersonal relatedness facilitate the development of new levels in the sense of self. In normal development these two developmental lines of self definition and interpersonal relatedness develop in a mutually facilitating and synergistic fashion (see Figure 1). Figure 1
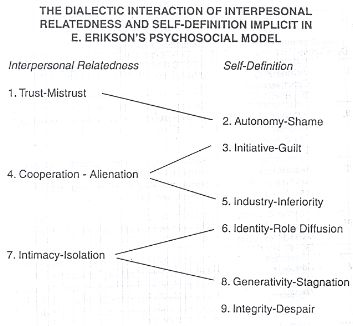
The dialectic synergistic development of concepts of self and of the relationship with others can be illustrated by an elaboration of Erikson's epigenetic model of psychosocial development. Erikson's (1950) model, though presented basically as a linear developmental process, implicitly provides support for the view that normal personality development involves the simultaneous and mutually facilitating development of self-definition and interpersonal relatedness. If one includes in Erikson's model an additional stage of mutuality versus alienation (occurring around the time of the development of cooperative peer play and the initial resolution of the oedipal crisis at about four to six years of age), and places this stage at the appropriate point in the developmental sequence, between Erikson's phallic-urethral stage of "initiative versus guilt" and his "industry versus inferiority" of latency (Blatt & Shichman 1983), then Erikson's epigenetic model of psychosocial development illustrates the complex transaction between interpersonal relatedness and self-definition that occurs in normal development throughout the life cycle (see Figure 2). Figure 2
Erikson initially emphasizes interpersonal relatedness in his discussion of trust versus mistrust, followed by two stages of self-definition, autonomy versus shame and initiative versus guilt. This is followed by the new additional stage of interpersonal relatedness, mutuality versus alienation, and then by two stages of self. definition, industry versus inferiority and identity versus role diffusion. The following stage, intimacy versus isolation, is again clearly a stage of interpersonal relatedness, followed by two more stages of self-definition, generativity versus stagnation and integrity versus despair (Blatt & Shichman 1983). This reformulation of Erikson's model (Blatt, 1990; Blatt & Blass, 1990, in press; Blatt & Shichman, 1983) corrects the deficiency noted by a number of theorists (e.g. Franz & White, 1985) that Erikson's model tends to neglect the development of interpersonal attachment. The articulation of an attachment developmental line broadens Erikson's model and enables us to note more clearly the dialectic developmental transaction between relatedness and self definition implicit in Erikson's developmental model. Relatedness and individuality (attachment and separation) both evolve through a complex interactive developmental process. The evolving capacities for autonomy, initiative, and industry in the individuality developmental line, develop in parallel with the development of a capacity for relatedness - to engage with and trust another, to cooperate and collaborate in activities with peers (e.g., play), to develop a close friendship with a same-sex chum, and to eventually experience and express feelings of mutuality, intimacy and reciprocity in an intimate, mature relationship. In normal development, there is a coordination between the evolving capacities along these two developmental lines. For example, one needs a sense of basic trust to venture in opposition to the need-gratifying other in asserting one's autonomy and independence, and later one needs a sense of autonomy and initiative to establish cooperative and collaborative relationships with others. Though these two developmental lines interact throughout the life cycle, they remain relatively independent of each other through the early developmental years. Subsequent levels of cognitive-affective schema, beginning with the development of concrete operational thought, involve the increased coordination and integration of these two developmental lines. Though addressing primarily the nature of the coordination of the relationship among dimensions of inanimate objects, Piaget's and Werner's identification of the development of concrete operational thought at about 6 years of age (Piaget, 1926/1955; Werner, 1948/1957; and Werner & Kaplan, 1963) identifies the emergence of a new cognitive schema in which the child is able to coordinate more effectively thc relationships among several dimensions. The child now understands the processes involved in the transformation of an object and has developed the capacity for appreciating reversibility and conservation. The beginning development of thc capacity for reversibility, transformation and conservation in operational thought at about thc age of 6 years, is consistent with the observations of psychoanalytic investigators of a major shift in the child, at about the age of 5, from a focus on a separate dyadic relationship with each parent alone, to the child's beginning appreciation of a triadic interpersonal structure and his/her role in a family system with contrasting and coordinating relationships with both parents. As a consequent of this awareness of triadic relationships, the child is increasingly able to consider interpersonal relationships in comparative terms. The child's thinking is no longer restricted to simple contrasts (e.g., pleasure-pain or issues of power, control and autonomy) that exist in a dyadic relationship, but the child can begin to reflect upon and compare and contrast the type and quality of the relationship he has with each of his parents and that the parents have with each other. Thinking is no longer just immediate, direct, and literal. Rather, qualities of self and others can be varied and reconstructed in new and complex ways. The child's new-found capacity for complex cognitive transformations results in a greater capacity for delay. Thus, affects increasingly have a signal or informational function rather than being primarily a stimulus for expressive discharge (Blatt, 1983). Thinking is no longer restricted to reproductions of concrete past experiences, but the child can begin to anticipate and plan for activities and events never experienced directly before (Piaget, 1945/1962). A full sense of time and of the future also emerge during this period (Loewald, 1960, 1962; Piaget, 1961/1969). The child not only has his own point of view, but now can also begin to appreciate the perspective of others and eventually realize that he/she is a unique person among all others, with a different and unique perspective (Feffer, 1959, 1970; Inhelder & Piaget, 1959/1964; Laurendeau & Pinard, 1962, 1970). Thus, the development, at around the age of 5 or 6, of what Piaget (1937/1954) calls operational thought, with its capacity for reversibility, transformation, and conservation, is cognitively essentially the same as the establishment of triadic interpersonal structures described by psychoanalytic theorists that occurs in the internalizations of the oedipal phase. The coordination and integration of aspects of individuality (or self definition) and relatedness at age 5 or 6, with the beginning resolution of the oedipal crisis and the advent of concrete operational thought, is expressed in an emerging sense of "we." George S. Klein (1976), in part derived from Erikson, stressed the importance of an integration of individuality and affiliation and its expression in the development of the concept of "we." G.S. Klein commented: One must feel "both separate and a part of an entity beyond itself... Identity must always be defined as having aspects of both separateness and membership in a more encompassing entity, and as developing functions that reflect one's role in a relationship with a larger entity" (pp. 178-179). G.S. Klein (1976) viewed psychoanalysis and much of psychology as having been predominantly concerned with a concept of self as a separate, autonomous unit and as not addressing the importance of the development of a sense of "belonging to" or of "we-ness." G.S. Klein argued for the need in psychoanalysis to include a concept of we that emerges from the dialectic between the development of a sense of self and a sense of relatedness to others (Blatt & Blass, 1990). Investigators, mainly in infant research, have begun to elaborate the conceptualization of this dialectic developmental process. Emde (1988) in discussing the dialectic between thc development of a sense of self and of relatedness, believed that the emergence of this dual emphasis is reflective of an important theoretical development: It is perhaps ironic that in our age, so preoccupied with narcissism and self, [that] we are beginning to sec a different aspect of psychology, a "we" psychology in addition to a "self" psychology. I draw our attention to the fact that this represents a profound change in our world view (Emde, 1988, p. 36). The profound change of which Emde spoke involves an expansion of concepts of the self-system to include the we dimension. Emde discussed three dynamic aspects of the self system: the experience of self, the experience of the other (e.g., attachment figure), and the experience of the self with other or we. A marked change occurs in the developmental process in adolescence. Beginning in adolescence, various components of self and others are integrated and coordinated further in a new gestalt or synthesis. The coordination of the two lines of development of concepts of self and of others in a concept of we, that was first expressed in concrete manifest terms with the beginning of operational thought at age 6, now occurs in more formal, abstract terms as the child begins to deal with complex internal psychological properties of the self and others in early adolescence, around the age of 11 or 12. The development of formal operational thought and the increased appreciation of internal psychological qualities, defines yet another level in the coordination and integration of concepts of self and other - of individuality and relatedness. This emphasis on integration in adolescence indicates a fundamental shift in the mechanisms of psychological development from internalization to integration (Blatt & Blass, 1990). Erikson (1968) noted this shift to integration as the fundamental developmental mechanism in adolescence in his description of the identity stage in adolescence as involving "the integration of the identity elements ascribed... to the childhood stages" (p. 128). He noted that Identity formation, finally, begins when the usefulness of identification ends. It arises from the selective repudiation and mutual assimilation of childhood identifications and their absorption in a new configuration... [into] a new, unique gestalt which is more than the sum of its part? (pp. 158-159). The successful outcome of the establishment of this new configuration is an integrated sense of self identity. Self identity, although partly a stage in the development of self definition, is also a cumulative, integrative stage in which the capacity to cooperate and share with others is coordinated with a sense of individuality that has emerged from the development of autonomy, initiative, and industry - the capacity for sustained goal-directed, task-oriented, activity. Self identity involves a synthesis and integration of individuality and relatedness - the internality and intentionally that develops as part of autonomy, initiative, and industry as well as the capacity and desire to participate in a social group with an appreciation of what one has to contribute co, and gain from, participating in the collective, without losing ones individuality within the collective or the relationship. Thus. in this sense, Erikson's more advanced stages of identity versus role diffusion, and integrity versus despair, are periods of a new and more complete synthesis of mature, integrated expressions of individuality and relatedness (Blatt & Blass, 1990, 1992 in press). The synthesis of these two developmental lines in an integrated self identity in adolescence leads to more mature expression of relatedness in intimate relationships characterized by mutuality and reciprocity, as well as to fuller expressions of individuality in generativity with sustained commitment to enduring values and goals. The integration of individuality and relatedness in self identity results in a capacity to establish a mutual and reciprocal relationship with another because one is now aware that (s)he has something unique and special to offer and share with the other. This awareness partly derives from a sense of self-worth, pride and competence that has previously emerged during the various earlier stages of the individuality developmental line as well as from an appreciation of the unique needs of the other. The capacity for intimacy also derives from a growing recognition of one's own needs and limitations, not only in what one has to offer the other, but also of the enrichment one can gain from the other and the pleasures in sharing and the advantages of reciprocity. Likewise, generativity, as formulated by Erikson, also involves a concern about extending beyond ones own self-interest and dedicating oneself to broader goals, values, and principles, including contributing to others and society. Thus, Erikson's stages of intimacy and generativity - the capacity to form a mutual and reciprocal relationship with another and to dedicate oneself to long-term principles and goals which extend beyond ones self interest - are both expressions of an integration of earlier developmental levels of individuality and relatedness that have been consolidated in a mature self-identity, a "self-in-relation" (Gilligan, 1982, 1989; Surrey, 1985), an "ensembled individualism" (Sampson, 1985, 1988), or a full sense of "we." In this sense, Erikson's more advanced stages of identity versus role diffusion and integrity versus despair are periods of integration of mature expressions of the relatedness and self-definitional developmental lines. Thus there is a shift in the mechani5ms of psychological development from internalization to integration (Blatt & Blass, 1990). Cognitive Schemas and Psychopathology in Adults The various levels of cognitive structures and schema from boundary articulation to integrity, initially established in an interpersonal context, are extended as generalized cognitive structures that are used to understand aspects of both the interpersonal and the impersonal world. As indicated by research on insecure attachment (e.g., Ainsworth, 1969, 1982; Bowlby, 1973, 1988; Bretherton, 1987; Main, Kaplan, & Cassidy, 1985), disruptions of caring relationships, at particular times in the life cycle, can lead to distortions in the development of these cognitive schema. Bowlby (1973, 1988) discussed how various developmental pathways, leading to mental health or to vulnerability to psychological disturbances, are determined by the quality of the attachment between parent and child. Though early caring experiences are quite significant and have considerable impact in determining developmental pathways, subsequent life experiences and interpersonal relationships can compound initial vulnerabilities or, as might occur within a psychotherapeutic relationship, may serve to ameliorate or compensate for earlier disruptions. Thus, these developmental pathways and impaired cognitive-affective or representational schemas are not necessarily fixed and immutable, but can be altered by subsequent experiences. But more often, however, these early cognitive-affective structures establish basic and fundamental developmental pathways that become consolidated and elaborated by subsequent experiences because individuals tend to seek out experiences that are congruent with their expectations and to interpret events based on previously established cognitive-affective schema (Buss, 1987). Because these cognitive schema are established initially in an interpersonal matrix, disturbances in cognitive schema will usually be apparent primarily in the intensity and ambiguity of interpersonal relationships and only secondary in more neutral conditions when dealing with inanimate objects and impersonal situations. A fundamental postulate of this paper is that a wide range of psychopathology that can occur in adults can be understood more fully as expressions of disruptions in the development of these various levels of cognitive-affective schema. A. Disturbances in Boundary Constancy and Schizophrenia Much of the symptomatology of schizophrenia such as hallucinations and delusions as well as disturbances in cognition, perception, attention, concept formation, and interpersonal relationships can be understood as expressions of disturbances in boundary articulation (Blatt & Wild, 1976; Blatt, Wild & Ritzler, 1975). It is impressive that a large number of clinical investigators over many years (e.g., Burnham, Gladstone, & Gibson, 1969; Federn, 1952; Freeman, Cameron & McGhie, 1966; Freud, 1929; Lidz, 1973; Lidz & Lidz, 1952; Searles, 1965; Tausk, 1919) have noted that schizophrenia involves disruption of one of the earliest and most fundamental cognitive-affective structures - the capacity to experience, perceive and represent a separation and differentiation between independent events and objects. These clinical investigators noted that poorly articulated and unstable boundaries occur primarily in more disturbed schizophrenic patients who have impoverished object relations, severely impaired capacities for adaptation, and a life history of estrangement and isolation. Disturbances in establishing and maintaining fundamental boundary distinctions in schizophrenia result in difficulty differentiating between people, so that people tend to be experienced as fused and confused with one another. Impaired boundary constancy makes it difficult to distinguish between self and non-self, between inside and outside, and between fantasy and reality. Lack of adequate boundary articulation results in diffuse and unarticulated perception in which there is an inability to differentiate figure from ground, an impaired capacity to maintain perceptual constancy, and failure to distinguish between separate images, concepts and experiences. Difficulty articulating boundaries also interferes with the capacity to maintain focused attention which results in severe distractibility, loose associations, and an inability to perceive accurately and to think logically (Blatt & Wild, 1976). Because of impaired boundary constancy, schizophrenic patients also have difficulty with recognition or libidinal constancy; they experience people, and reality more generally, as unstable and fluid. Thus, they have difficulty maintaining a sense of relatedness. With interpersonal stress, schizophrenic patients often withdraw investment in interpersonal relationships and retreat instead into autistic fantasies as a replacement for unstable, painful and dangerous interpersonal relationships (Blatt, Brenneis, Schimek, & Glick, 1976b; Blatt, Schimek, & Brenneis, 1981). Thc formulation of schizophrenia as involving a fundamental disturbance in boundary schema and recognition or libidinal constancy not only provides a frame. work for integrating a large segment of the vast research literature on the disruptions of cognitive, perceptual and interpersonal processes of schizophrenic patients (Blatt & Wild, 1976), but it also provides fuller understanding of paranoid schizophrenia. More intact paranoid schizophrenic patients struggle, in exaggerated ways, to preserve a sense of boundaries. Paranoid schizophrenic patients not only have greater differentiation and more sharply delineated boundaries than non-paranoid schizophrenic patients, but they have significantly greater differentiation than even normals (Freeman et al., 1966; Shakow, 1962; Witkin, 1965). The paranoid schizophrenic patient's heightened sense of cognitive control, exaggerated perceptual articulation, hyper-alert attention, emphasis on part properties and on differences between self and others, express an exaggerated defensive struggle to preserve and solidify boundaries (Blatt &Wild, 1976). A preoccupation with power, control and autonomy, excessive su5piciousness, the isolation of affect, and keeping people at a distance because they are dangerous and threatening, are attempts to maintain rigidly a sense of individuation and separation and to defend against the threat of boundary dissolution and experiences of merger and fusion. B. Disturbances in Evocative Constancy and Borderline Personality Disorder Clinical and research findings indicate that borderline patients have particular impairment not in boundary schema or libidinal (recognition) constancy, but in evocative constancy (e.g., Adler & Buie. 1979; Blatt & Auerbach, 1988; Blatt & Shichman, 1983). The vulnerability of borderline patients to feeling rejected and abandoned and their profound reactions to separation and loss, suggest an impairment in evocative constancy - in the ability to establish and sustain an enduring sense of self and of a sense of relatedness with significant others during stressful moments (Blatt & Auerbach, 1988). When a significant relationship is disrupted or threatened, the borderline patient experiences the other not only as disinterested or unavailable, but as completely lost. Profound feelings of abandonment, reaction and aloneness disrupt the borderline patients capacity for reality testing. Disturbances in evocative constancy in borderline patients are also expressed in an inability to maintain a cohesive and effective sense of self in the face of criticism or rejection (Kohut, 1977). Disapproval and criticism result in feelings of fragmentation or depletion of the self. Cognitive processes become fragmented, idiosyncratic and illogical (Blatt & Auerbach, 1988). Dramatically vivid, exaggerated and polarized concepts, intense idealization and gross denigration, typically characteristic of borderline patients, can best be understood as desperate attempts to maintain a sense o( relatedness to and contact with others, especially when borderline patients feel vulnerable. Borderline patients are vulnerable to disorganization as a consequence of experiences of abandonment and stress because their mental representations or cognitive-affective schemas of self and other lack sufficient structure to provide coherent and organized patterns of attachment to cope with feelings of loneliness and loss. The flamboyant cognitive and behavioral features and the affective storms of borderline personality disorders reflect exaggerated efforts to sustain interpersonal contact. Exaggerated, overstated images and behavioral expressions are an attempt to vivify experiences and mental representations to compensate for a deficit in evocative constancy and overcome intense feelings of emptiness, aloneness, abandonment. worthlessness, fragmentation, and/or rage (Adler & Buie, 1979; Gunderson, 1984; Kernberg, 1975; Kohut, 1977; Masterson & Rinsley, 1975). Because deficits in evocative constancy are central to borderline character pathology, unstructured situations are highly stressful for borderline patients. The lack of structure of Rorschach stimuli and of psychological testing, more generally (Arnow & Cooper, 1984), for example, confronts directly the impaired capacity for evocative constancy of borderline personalities. Greater environmental structure, in contrast, enables the borderline personality to contain their impaired evocative constancy and to function more effectively. Thus, for example, on the well-structured Wechsler Adult Intelligence Scale (WAIS) patients with borderline character disturbance usually function without apparent disturbance. But because evocative constancy is necessary to organize and guide behavior when environmental structure and definition are reduced or absent, the functioning of borderline patients declines dramatically when situations and tasks are ambiguous (Blatt & Auerbach, 1988). C. Self and Object Constancy and the Neuroses Personality development subsequent to the establishment of evocative object and self constancy between 16 months and 3 years of age occurs as a complex dialectical transaction between two fundamental developmental lines: 1) the development of a consolidated, realistic, essentially positive, increasingly differentiated and integrated self definition or identity, and 2) the development of the capacity to establish increasingly mature, reciprocal, and satisfying interpersonal relations. Normally, these two developmental lines develop in a mutually facilitating fashion. An increasingly differentiated, integrated, and mature sense of self is contingent upon establishing satisfying interpersonal experiences, and, conversely, the continued development of increasingly mature and satisfying interpersonal relationships is contingent upon the development of a more mature self-definition and identity. Meaningful and satisfying relationships contribute to the evolving concept of the self, and a new sense of self leads, in turn, to more mature levels of interpersonal relatedness. In normal personality development, these two developmental processes evolve in an interactive, reciprocally balanced, mutually facilitating way (Blatt, 1990; Blatt & Blass, 1990; Blatt & Shichman, 1983). As indicated by attachment research, secure attachment involves both a capacity to establish affective bonds and to tolerate and benefit from separation. Secure attachment results in the simultaneous and synergistic development of concepts of self and of relations with others that facilitates the development of increasingly mature levels of interpersonal relatedness and of autonomy and individuation as expressed in the development of the capacity both to love and to work (Hazen & Shaver, 1990). On occasion, some individuals experience severe disruptions of this normally developing dialectic process of self definition and interpersonal relatedness. Attempts to cope with these serious developmental disruptions often result in some individuals placing an exaggerated emphasis on one of these dimensions while defensively avoiding the other. Exaggerated and distorted emphasis on self definition or on relatedness to others can occur at different developmental stages and be expressed in different stage-specific preoccupations. These formulations are consistent with evidence from attachment research that indicates that insecure attachment results in either a preoccupation with relatedness (anxious ambivalent insecure attachment) or in an exaggerated and distorted emphasis on separation (avoidant insecure attachment). This distorted emphasis in insecure attachment patterns interferes with the synergistic dialectic interchange between relatedness and self definition that is essential for normal development. But it is important to stress that the insecure attachment patterns do provide a coherent structure (or representing consistent and stable concepts of self and others, even if in less than optimal ways. Evidence suggests that patterns of insecure attachment predispose an individual to various forms of psychopathology, especially depression. Bowlby (1977, 1980, 1988) and Sroufe (1983), for example, have noted a vulnerability to depression in anxiously ambivalent (or preoccupied) insecurely attached individuals, who are overly dependent on interpersonal contact because of their experience of early inconsistent and unreliable care-taking, as well as in compulsively self-reliant or avoidant individuals who shun interpersonal contact because of experiences with punitive and intrusive caretakers. Blatt and his colleagues (Blatt, 1974; Blatt & Homann, 1992; Blatt & Maroudas, 1992; Blatt & Zuroff, 1992) noted that the two patterns of insecure attachment may cach be associated with a different type of depression. Preoccupied insecure attachment appears to be associated with a dependent (Blatt, D'Afflitti & Quinlan, 1976), anaclitic (Blatt, 1974), sociotropic (Beck, 1983) type of depression that is precipitated by disruptions of interpersonal relations and experiences and fears of abandonment and loneliness. Avoidant insecure attachment appears to be associated with a self critical (Blatt et al., 1976), introjective (Blatt, 1974), autonomous (Beck, 1983) type of depression that is precipitated by a loss of self-esteem and characterized by feelings of worthlessness, blame, and guilt. Experiences in the dependent type of depression are often expressed in a sensorimotor-preoperational (Blatt, 1974) or enactive (Bruner, 1964; Horowitz, 1972) mode, while experiences in a self-critical depression are often represented in a more imagistic (Bruner, 1964; Horowitz, 1972) or concrete perceptual or external iconic (Blatt, 1974) mode in which specific perceptual features and or behaviors (gestures or acts) are used to represent particular feelings and thoughts (Blatt, Wein, Chevron & Quinlan, 1979). Patterns of preoccupied and avoidant insecure attachment have also been identified in adolescents and adults by several research groups (e.g., Shaver & Hazen, 1987; West & Sheidon, 1988). Malcolm West and his colleagues, primarily from a clinical perspective, discussed how a preoccupation with relatedness can be expressed in either compulsive care-seeking or compulsive care-giving. Other investigators, such as Shaver and Hazan (1987) and Bartholemew and Horowitz (1991), primarily from a social psychological perspective and using somewhat different concepts and measures, demonstrated how a preoccupation with separation and aloneness can be expressed in either a dismissive or a fearful avoidant attachment style. Thus, the preoccupied and avoidant patterns of insecure attachment, identified in infant research as a basic style that emerges with the consolidation of evocative constancy at about 16 months of age, appear to have continuity throughout the life cycle. The identification of preoccupied and avoidant patterns of insecure attachment in infants, children, adolescents and adults, not only identifies two basic types of insecure attachment, but the findings with adolescents and adults suggest that there may be several different developmental levels within each of these two broad patterns of insecure attachment. There appears to be two types or levels of preoccupied (anxious-ambivalent) insecure attachment in which compulsive care-giving may be a more mature and integrated expression of the preoccupied attachment style in contrast to less mature, unilateral, non-reciprocal pattern of compulsive care-seeking (see Blatt, Zohar, Quirtian, Zuroff & Mongrain, in press). The compulsive caregiver provides care in the way s/be wants to bc cared for (Blatt et al., 1982) and therefore this style may leave greater potential for establishing reciprocity and mutuality in providing as well as receiving care and affection. Compulsive care-seekers, in contrast, seem less mature because they primarily seek unilateral relationships that provide contact, nurturance, gratification, support, approval and acceptance from others. Carrie Schaffcr (1993) of our research group at Yale in a sample of non-clinical young adults, found that compulsive care-seekers reported significantly greater levels of dependency, self-criticism and anxiety, as well as a lower level of self-efficacy than did compulsive caregivers. In terms of modes of affect regulation, she found that compulsive care-seekers report using significantly more oral/somatic expressions and more frequent use of images of sex and aggression to modulate their affects, while compulsive caregivers report significantly greater use of cognitive processes and interpersonal involvement as modes of affect regulation. A similar developmental differentiation seems possible within avoidant insecure attachment, as indicated by Bartholemew's (1990) recent distinction between a dismissive and a fearful avoidant pattern within avoidant insecure attachment (see also Brennan & Shaver, 1990). Bartholemew found that fearfully avoidant subjects are characterized by a conscious desire for relatedness that is inhibited by fears of its consequences. Fearful subjects are low in self-esteem, hesitant, shy, lonely, vulnerable, dependent, self-critical, afraid of rejection, and lacking in social confidence. On the other hand, dismissive avoidant subjects are characterized by an intense defensive denial of the need and/or desire for relatedness. They rate themselves as high in self esteem, socially self-confident, unemotional, independent, cynical, critical of and distant from others, and more interested in achievement than in interpersonal relationships. Although dismissing avoidant subjects rate themselves as high in self-esteem, their peers viewed them as hostile, socially autocratic, and less ego resilient (Kobak & Sceery, 1988). Thus, dismissive avoidance may represent a less integrated and adaptive expression of the avoidant attachment style than the fearful avoidant pattern. Ken Levy of our research group at Yale (Levy et al., in press), using Bartholemew's measure to differentiate fearfully avoidant and dismissively avoidant subjects, studied the quality of these subjects' representations of their mothers and fathers. [Footnote 2: Levy et al. also found that secure subjects are less ambivalent about their parents and described both their mother and father as more benevolent, warm, affectionate, non-judgmental and non-punitive, and as a positive idea[ who is nurturing and constructively involved, than did insecure subjects. Secure subjects also appear to grasp more fully the complexity of relationships and to differentiate themselves more fully from their parents which still being able to maintain of sense of relatedness. Within the insecure groups, Levy found that avoidant subjects described their parents as generally cold, judgmental, punitive, and less constructively involved. Anxious ambivalent subjects, in contrast, described their parents as punitive and judgmental, but also as affectionate, warm, and benevolent, as well as generally ineffective - less successful, less constructively involved, and less of a positive ideal. Both avoidant and anxious ambivalent insecure subjects expressed significantly more ambivalence about their parents than secure subjects.] Fearful avoidant subjects expressed significantly greater ambivalence when describing their parents than dismissively avoidant subjects, primarily because the dismissively avoidant subjects de5cribe their parents in polarized terms as either generally punitive, malevolent and lacking warmth, or as highly idealized. The descriptions of parents by dismissively avoidant subjects, as compared to fearfully avoidant subjects, were significantly less differentiated and conceptually less complex. While fearful avoidant subjects, in contrast, represented their parents as more malevolent and punitive, their descriptions were more differentiated and at a higher conceptual level. Although fearful subjects have highly ambivalent and more negative representations of their parents, they see the complexity of relationships and differentiate themselves more fully from their parents than dismissively avoidant subjects. Thus, like with preoccupied insecure attachment, we seem to be able to differentiate two developmental levels within the avoidant insecure attachment style. Within the preoccupied group, compulsive caregivers appear to bc developmentally more mature than compulsive care-seekers; and likewise within the avoidant group, fearfully avoidant subjects appear to be at a higher developmental level than dismissive avoidant subjects. Thus, the differentiation between the two types of insecure attachment, avoidant or preoccupied, appears to define two basic styles of insecure attachment, and within each of these two broad types of insecure attachment there appears to be a least two different developmental levels. These distinctions both between and within the two insecure attachment styles are consistent with and provide empirical support for the formulations of Blatt and his colleagues (Blatt, 1974, 1990; Blatt & Biass, 1990, 1992; Blatt & Shichman, 1983) who distinguish an anaclitic personality style that occurs as a' consequence of preoccupation with issues of interpersonal relatedness and an initrojective personality that occurs as a consequence of an emphasis on issues of self definition. Normal development, like secure attachment, involves an integrated and coordinated development of the capacity (or establishing mature levels of interpersonal relatedness and an essentially positive and realistic sense of self. Emphasis on issues of relatedness or self definition appear to delineate two basic personality configurations, each with a particular experiential mode and preferred forms of cognition, defense, and modes of adaptation (Blatt, 1990; Blatt & Shichman, 1983). Which of these two tendencies receives priority (Maddi, 1980) appears to define important differences in personality style and motivational dispositions (Bakan, 1966). Attachment theory and research, suggest that these two general personality styles may result from different types of care-giving experiences (see also Blatt & Homann, 1992, and Blatt & Zuroff, 1992). Individuals who place a relatively greater emphasis on interpersonal relatedness are generally more figurative in their thinking and usually focus primarily on affects and visual images. Their thinking is characterized as more simultaneous than sequential and they emphasize reconciliation, synthesis, and integration of elements rather than the critical analysis of separate elements and details. In terms of cognitive style, these individuals tend to be primarily field dependent. They seek fusion, harmony, integration, and synthesis and are interested more in feelings, affects, and personal reactions rather than facts, figures, and details. Their primary instinctual mode is libidinal rather than aggressive, and they value affectionate feelings and thc establishment of close intimate relationships (Blatt & Shichman, 1983). Thinking in individuals primarily focused on self definition is more literal, sequential, linguistic, and critical. Overt behavior, manifest form, logic, consistency, and causality are attended to rather than feelings and relationships. Emphasis is on analysis rather than synthesis, on the critical dissection of details and part properties rather than on achieving integration and synthesis. These individuals tend to be field independent (Witkin, 1965; Witkin, Dyk, Faterson, Goodenough, & Karp, 1962). Their primary goal is self assertion, control, autonomy, power, and prestige and their primary instinctual mode involves assertion and aggression in the service of differentiation and self-definition rather than affection and intimacy (Blatt, 1990; Blatt & Shichman, 1983). These two personality styles are also associated with two different types of depressive experiences (e.g., Blatt et al., 1976; Blatt, Quinian, Chevron, McDonald & Zuroff, 1982). This exaggerated emphasis on either relatedness or on isolation and self definition in. the extreme also provides a basis for distinguishing different types of psychopathology, especially in the neurotic range. As indicated in Figure 3, various types of psychopathology can be defined as involving a distorted preoccupation with issues of relatedness or with issues of self-definition at different developmental levels. Figure 3
Disorders in which there is an exaggerated and distorted emphasis on interpersonal relatedness and defensive avoidance of issues of self definition (anaclitic disorders) include the infantile character and hysterical disturbances. Disorders which place an exaggerated and distorted emphasis on defining a sense of self and defensive avoidance of issues of relatedness include paranoia, obsessive-compulsive disorders, introjective (guilt-ridden) depression, and phallic narcissism (introjective disorders). Thus, there appears to be two major configurations of neurotic psychopathology, one in which there is an excessive preoccupation with issues of relatedness and the other with issues of separation and self definition. These two configurations of psychopathology are consistent with the two types of insecure attachment that emphasize an exaggerated dependency on others or on angry isolation and compulsive self-reliance (Blatt, 1974,1990; Blatt & Shichman, 1983). The infantile character and the hysteric are both excessively concerned about bonding and relatedness. At a more primitive level, the infantile character is concerned about being cared for, while at a higher developmental level the hysteric is concerned about establish mutual relationships - wanting to love as well as to be loved. But both these disorders are concerned about bonding and libidinal attachment. Some patients are primarily at the infantile level, other patients are predominantly at the hysteric level, but most of these patients who are intensely concerned about relatedness move back and forth along a developmental continuum of interpersonal relatedness. Thus, many patients will have a blend of infantile and hysteric features and will vary on this continuum depending upon the level of stress they are experiencing and their capacity to manage it. But infantile and hysterical disorders ac interrelated forms of psychopathology and nor separate disease entities. Oedipal themes of the hysteric are often found in infantile character disorders, and oral themes of the infantile character are often found in the hysteric. It is not uncommon to find a blend of oral and genital psychosexual preoccupations (Marmor, 1953) because both of these libidinal preoccupations involve interpersonal relatedness. The same is true of introjective psychopathologies. Paranoia, obsessive-compulsive disorders, introjective depression, and phallic narcissism are all attempts, in more or less primitive ways, to protect and define a sense of self. The paranoid patient's preoccupation with power and self-justification is a primitive attempt to preserve a sense of self-definition. Obsessive patients are also concerned about self-definition but at a somewhat more mature level, as expressed in concerns about maintaining control and their prerogatives, rights, possessions, words, and ideas. A patient with an introjective (guilt-ridden) depression is also concerned about self-definition as expressed in exaggerated feelings of guilt, transgression, wrong- doing and failure. Phallic narcissism is the reciprocal of introjective depression in that the individual takes excessive pride in the self and his/her accomplishments. Others are simply an audience to observe and applaud his grandiose accomplishments. These different forms of introjective psychopathology (paranoia, obsessive- compulsive, guilt-ridden depression, and phallic narcissism) are not separate disease entities, but are interrelated modes of adaptation. Paranoid parents often have significant obsessive features and are defending against powerful feelings of depression and guilt. Likewise, obsessive patients can regressively decompensate and develop paranoid features and the same is true of someone with a guilt-ridden depression. Thus, introjective forms of psychopathology are interrelated modes of adaptation that occur at different developmental levels along a single continuum. Individual patients can function predominantly at a particular developmental level and progress or regress along this continuum depending on a variety of circumstances. Ali these introjective disorders share an emphasis on aggression, directed at others or the self. They are much more concerned about self-assertion and aggression than about bonding and relatedness (Blatt, 1990; Blatt & Blass, 1990; Blatt & Shichinan, 1983). These two groups or configurations of disorders, anaclitic and introjective, differ not only in terms of basic instinctual focus (libidinal versus aggressive), but they also differ in terms of basic defense mechanisms. Anaclitic disorders involve primarily avoidant defenses (e.g., denial and repression) while introjective disorders involve primarily counteractive defenses (e.g., projection, intellectualization, reaction formation, overcompensation). These formulations of two primary configurations of psychopathology have not only proven to be particularly useful in studies of depression (Blatt & Maroudas, 1992; Blatt & Zuroff, 1992) but they have been important differentiations in the study of therapeutic change (Blatt, 1992; Blatt & Ford, 1994; Blatt, Ford, Berman, Cook & Meyer, 1988). Therapeutic change was studied in a large sample of seriously disturbed patients who were in long-term, intensive, psychoanalytically oriented, inpatient treatment in an open therapeutic facility (Blatt & Ford, 1994; Blatt et al., 1988). Systematic differences were found in independent measures of behavioral and psychological change after 15 months of intensive inpatient treatment (including 4 times weekly psychoanalytically oriented psychotherapy) between patients preoccupied primarily with concerns about disruptions of interpersonal relatedness (anaclitic patients) and those preoccupied primarily with issues of self-definition, autonomy, self-control and self-worth (introjective patients). Introjective patients seemed to change more readily and to express their improvement primarily in a reduction of clinical symptoms as reliably rated from case reports, and in increases in cognitive functioning as independently assessed on psychological tests administered at the beginning and toward the end of treatment (significant diminution of thought disorder on the Rorschach and an elevation o( intelligence). Therapeutic change seemed to occur more slowly and in more subtle form in anaclitic patients and expressed primarily in changes in the quality of interpersonal relationships as reliably rated from case reports and in their representation of the human figure on the Rorschach. Thus, anaclitic and introjective patients appear to change primarily in the modalities that express their respective basic concerns and preoccupations. A second study re-examined the data gathered as part of the Menninger Psychotherapy Research Project (MPRP). The MPRP was designed to compare the effects of psychoanalysis and long-term psychodynamically oriented psychotherapy in the treatment of outpatients (Blatt, 1992). Despite many prior analyses of various dimensions of data derived from clinical evaluations and psychological testing conducted before and after treatment, the results of the MPRP have repeatedly failed to discern any differences between two different types of therapeutic intervention (Wallerstein, 1986). Reanalysis of the data from the MPRP utilizing the distinction between the two configurations of psychopathology, however, indicated that anaclitic and introjective patients are differentially responsive to psychotherapy and psychoanalysis. Based on recently developed procedures for systematically evaluating the quality of object representation on the Rorschach (Blatt, 1990b; Blatt & Berman, 1984), independent analysis of the psychological test data gathered at the beginning and at the end of treatment as part of the M PRP revealed that anaclitic patients had significantly greater positive change in psychotherapy than in psychoanalysis, while introjective patients had significantly greater positive change in psychoanalysis than in psychotherapy. Thus, the relative therapeutic efficacy of psychoanalysis versus psychotherapy seems contingent to a significant degree upon the nature of the patients pathology and character structure. It seemed consistent that more dependent, interpersonally oriented patients would respond more effectively in a therapeutic context in which there is more personal interaction with the therapist. It also seemed consistent that more ideational patients who stress their individuation, autonomy, and independence respond more effectively in psychoanalysis. These statistically significant patient-by-treatment interactions indicate the importance of differentiating among these two types of patients in studies of therapeutic outcome and of therapeutic process. Congruence between. patients' character style and important aspects of the therapeutic situation appear to determine the nature and efficacy of treatment outcome. This reanalysis of the data of the MPRR consistent with the findings of the first study, indicates the importance of including distinctions between anaclitic and introjective patients in evaluating dimensions of therapeutic change. Patients come to treatment with different types of problems, different character styles, and different needs, and are responsive in different ways to different types of therapeutic intervention (Blatt & Felsen, 1993). The differential response of anaclitic and introjective patients in these two studies of therapeutic change and outcome in long-term treatment, suggests that this distinction may bc useful when systematically evaluating the differential effectiveness of various forms of brief psychotherapy (e.g. cognitive-behavioral as compared to interpersonal therapy) in treating depression. The NIMH Treatment of Depression Collaborative Research Project (TDCRP) (e.g., Elkin et al., 1989) compared three forms of treatment for depression (interpersonal therapy [IPT], cognitive behavioral therapy [CBT], and imipramine plus clinical management). In the primary analysis of their data, these investigators found "no evidence of greater effectiveness of one of the psychotherapies as compared with the other and no evidence that either of the psychotherapies was significantly less effective than... imipramine plus clinical management" (Elkin et al., 1989, p. 971). Interpersonal psychotherapy and imipramine plus clinical management, however, were more effective than cognitive-behavioral therapy with severely depressed patients who were functionally impaired. In an attempt to bring more precision to their research, Imber and his colleagues (Imber et al., 1990), in a further analysis of the NIMH TDCRP, argued for the need to develop measures of change that are directly relevant to possible treatment-specific effects. They stressed the need to develop precisely specified, appropriately applied, outcome measures "selected for presumed sensitivity to different treatments." Though these investigators carefully derived outcome measures based on the rationales and procedures of three types of treatment for depression (IPT, CBT, and imipramine plus clinical management), their results provide little support for their basic hypothesis: "None of the therapies produced consistent effects on measures related to its theoretical origin? (p. 352). Their findings appear to support the contention (Butler & Strupp, 1986) that the search for specific versus non-specific treatment effects is unproductive and that psychotherapy research should move on to more productive areas. Treatment effects, however, may occur as a consequence of patient dimensions rather than of aspects of the treatment process. The most recent analysis of the data from thc NIMH TDCRP (Sotsky et al., 1991) identified several patient characteristics that were predictive of treatment outcome. Higher social functioning predicted a generally favorable outcome (completion of treatment and severity of depression at termination) and a specific positive responsiveness to IPT. Higher cognitive functioning also appeared to predict good prognosis, but especially to CBT (reduction of depression severity). Patients with both impaired social and work functioning responded best to imipramine and clinical management (reduction of depression severity and completion of treatment). The results led the authors to suggest that "each psychotherapy relies on specific and different learning techniques to alleviate depression, and thus each may depend on an adequate capacity in the corresponding sphere of patient function to produce recovery with the use of that approach" (Sotsky et al., 1991, p. 1006). Patients with relatively good social functioning were better able to take advantage of interpersonal strategies in IPT in order to recover from depression, while patients with relatively less cognitive impairment were more able to utilize cognitive-behavioral techniques to reduce depression. These findings from the NIMH TDCRP are consistent with the results of the study of anaclitic and introjective patients in the MPRP, in which anaclitic patients, those with greater investment in interpersonal relatedness, showed greater improvement in psychotherapy, while introjective patients, those with greater investment in cognitive functioning, showed greater improvement in psychoanalysis. The fact that more ideational patients did better in psychoanalysis in the MPRP and in CBT in the NIMH TDCRP suggests that both short-term CBT and long-term psychoanalysis both emphasize change in cognitive structures, in contrast to the interpersonal emphasis of short-term IPT and long-term psychotherapy which was more effective with more interpersonally oriented patients. In summary, there appears to be considerable advantage in formulating various types of psychopathology as the result of impairments in the development of cognitive-affective schema or representational structures. Developmental theory provided a basis for differentiating various milestones in the development of cognitive-affective schema that appear to be congruent with manifestations of various major forms of psychopathology in adults. These formulations enable us to understand various forms of psychopathology not as separate and discrete illnesses or diseases, each characterized by a series of inconsistent and overlapping manifest symptoms, but as particular modes of maladaptation that occur as a consequence of disruptions in the development of cognitive-affective schema along a continuum ranging from more to less primitive levels of organization. These formulations of psychopathology in adults from a developmental perspective not only have heuristic value in providing a more reliable and valid way of establishing differential diagnoses in both clinical practice and research, but they may also provide more precise articulation of some of the psychological and interpersonal factors that lead to the formation of various types of psychopathology in adults. REFERENCES Abelson, R.P. (1981). Psychological states of the script concept. American Psychologist, 36, 715-729. Adier, G., & Buie, D.H., Jr. (1979). Aloneness and borderline psychopathology: The possible relevance of child development and issues. International Journal of Psycho-Analysis, 60, 83-96. Ainsworth, M.D.S. (1969). Object relations, dependency, and attachment: A theoretical review of the mother-infant relationship. Child Development, 40, 969-1025. Ainsworth, M.D.S. (1982). Attachment: Retrospect and prospect. In: C.M. Parkes & J. Stevenson-Hinde (Eds.), The place of attachment in human behavior (pp. 3-30). New York: Basic Books. Anderson, J.R. (1983). The architecture of cognition. Cambridge: Harvard University Press. Arnow, D., & Cooper, S.H. (1984). The borderline patient's regression on the Rorschach: An object-relations interpretation. Bulletin of the Menninger Clinic, 48, 25-36. Bakan, D. (1966). The duality of human existence: An essay on psychology of Religion. Chicago: Rand McNally. Bartholomew, K. (1990). "Attachment styles in young adults: Implications of self-concept and interpersonal functioning." Unpublished Doctoral Dissertation. Stanford University, Palo Alto, CA. Bartholomew K., & Horowitz, L. (1991). A four category model of attachment. Journal of Personality and Social Psychology, 61, 226-241. Beck, A.T. (1983). Cognitive therapy of depression: New perspectives. In: P.J. Clayton & J.E. Barrett (Eds.), Treatment of depression: Old controversies and new approaches (pp. 265-290). New York: Raven. Behrends, R.S., & Blatt, S.J. (1985). Internalization and psychological development throughout the life cycle. Psychoanalytic Study of the Child, 40, 11-39. Bell S.M. (1970). The development of the concept of object as related to infant-mother attachment. Child Development, 41, 292-311. Blatt, S.J. (1974). Levels of object representation in anaclitic and introjective depression. The Psychoanalytic Study of the Child, 24, 107-157- Blatt, S.J. (1983). Narcissism and egocentrism as concepts in individual and cultural development. Psychoanalysis and Contemporary Thought, 6, 291-303. Blatt, S.J. (1990a). Interpersonal relatedness and self-definition: Two personality configurations and their implication for psychopathology and psychotherapy. In: J.L. Singer (Ed.), Repression and dissociation: Implications for personality theory, psychopathology and health (pp. 299-335). Chicago: University of Chicago Press. Blatt, S.J. (1990b). The Rorschach: A test of perception or an evaluation representation. Journal of Personality Assessment, 55, 394-416. Blatt, S.J. (1991a). A cognitive morphology of psychopathology. Journal of Nervous and Mental Disease, 179, 449-458. Blatt, S.J. (1991b). Depression and destructive risk-taking behavior in adolescence. In: L.P. Lipsitt & L.L. Mitnick (Eds.), Self-regulatory behavior and risk taking: Causes and consequences (pp. 285-309). Norwood, NJ: Ablex Press. Blatt, S.J. (1992). The differential effect of psychotherapy and psychoanalysis on anaclitic and introjective patients: The Menninger Psychotherapy Research Project Revisited. Journal of the American Psychoanalytic Association. && Blatt, S.J., & Auerbach, J.S. (1988). Differential cognitive disturbances in three types of "borderline" patients. Journal of Personality Disorders, 2, 198-211. Blatt, S.J., & Berman, W. (1984). A methodology for the use of the Rorschach in clinical research. Journal of Personality Assessment, 48, 226-239- Blatt, S.J., & Blass, R.B. (1990). Attachment and separateness: A dialectic model of the products and processes of psychological development. The Psychoanalytic Study of the Child, 45, 107-127. Blatt, S.J. & Blass, R.B. (1992). Relatedness and self-definition: Two primary dimensions in personality development, psychopathology, and psychotherapy. In: J. Barron, M. Eagle, & D. Wolitzky (Eds.), The interface between psychoanalysis and psychology (pp. 399-428) Washington, DC: American Psychological Association. Blatt, S.J., & Blass, R. (in press). Relatedness and self-definition: A dialectic model of personality development. In: G.G. Noam & K.W. Fischer (Eds.), Development and Vulnerabilities in Close Relationships. Hillsdale, NJ: Lawrence Erlbaum Associates. Blatt, S.J., Brenneis, C.B., Schirnetk, J., & Glick, M. (1976a). "A developmental analysis of the concept of the object on the Rorschach." Unpublished research manual, Yale University. Blatt, S.J., Brenneis, C.B., Schimck, J., & Glick, M. (1976b). Normal development and psychopathological impairment of the concept of the object on the Rorschach. Journal of Abnormal Psychology, 85, 364-373. Blatt, S.J., D'Afflitti, J.P., & Quinian, D.M. (1976). Experiences of depression in normal young adults. Journal of Abnormal Psychology, 85, 383-389. Blatt, S.J. & Feisen, 1. (1993). "Different kinds of folks may need different kinds of strokes": The effect of patients' characteristics on therapeutic process and outcome. Psychotherapy Research, 3, 245-259. Blatt, S.J. & Ford. R.Q. (1994). Therapeutic Change: An Object Relations Perspective. New York: Plenum. Blatt, S.J., Ford, R.Q., Berman, W., Cook, B., & Meyer, R. (1988). The Assessment of Change During the Intensive Treatment of Borderline and Schizophrenic Young Adults. Psychoanalytic Psychology, 5, 127-158. Blatt, S.J., & Homann, E. (1992). Parent-Child interaction in the etiology of dependent and self-critical depression. Clinical Psychology Review, 12. 47-91- Blatt, S.J., & Lerner, H.D. (1983a). Investigations on the psychoanalytic theory of object relations and object representations. In: J. Masling (Ed.), Empirical studies of psychoanalytic theories, Vol. 1 (pp. 189-249). Hillsdale: NJ: Analytic Press. Blatt, S.J., & Lerner, H.D. (1983b). The psychological assessment of object representation. Journal of Personality Assessment, 47, 7-28. Blatt, S.J., & Lerner, H. (1991). Psychoanalytic perspectives on personality theory. In: M. Hersen, A. Bellack, J.A.E. Kazdin (Eds.), Handbook of Clinical Psychology, Revised Edition (pp. 147-169). New York: Pergamon Press. Blatt, S.J., & Maroudas, C. (1992). Convergence of psychoanalytic and cognitive behavioral theories of depression. Psychoanalytic Psychology, 9, 157-190. Blatt, S.J., Quinian, D. M., Chevron, E. S., McDonald, C., & Zuroff, D. (1982). Dependency and self-criticism: Psychological dimensions of depression. Journal of Consulting and Clinical Psychology, 50, 113-124. Blatt, S.J., & Shichman, S. (1983). Two primary configurations of psychopathology. Psychoanalysis and Contemporary Thought, 6, 187-254. Blatt, S.J., Wein, S.J., Chevron, E.S., & Quinlan, D.M. (1979). Parental representations and depression in normal young adults. Journal of Abnormal Psychology, 88, 388-397. Blatt, S.J., & Wild, C.M. (1976). Schizophrenia: A developmental analysis. New York: Academic. Blatt, S.J., Wild, C.M., & Ritzler, B.A. (1975). Disturbances of object representations in schizophrenia. Psychoanalysis and Contemporary Science, 4, 235-288. Blatt, S.J., Zobar, A.H., Quinian, D.M., Zuroff, D.C., & Mongrain, M. (in press). Subscales of attachment within the dependency factor of the Depressive Experiences Questionnaire. Journal of Personality Assessment.&& Blatt, S.J., & Zuroff, D.C. (1992). Interpersonal relatedness and self-definition: Two prototypes for depression. Clinical Psychology Review, 12, 527-562. Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. New York: Basic Books Bowlby, J. (1973). Attachment and loss, Vol. 2: Separation, anxiety, and anger. New York: Basic Books. Bowlby, J. (1977). The making and breaking of affectionate bonds: I. Etiology and psychopathology in light of attachment theory. British Journal of Psychiatry, 130, 201-210. Bowlby, J. (1980). Attachment and loss, Vol. 3: Loss, separation and depression. New York: Basic Books. Bowlby, J. (1988). Developmental psychiatry comes of age. American Journal of Psychiatry, 145, 1-10. Brennan, K.A., & Shaver, P.R. (1990). "Dimensions of adult attachment and the dynamics of romantic relationships." Unpublished manuscript, Department of Psychology, State University of New York at Buffalo. Bretherton, I. (1985). Attachment theory: Retrospect and prospect. In: I. Bretherton & E. Waters (Eds.), Growing Points in Attachment, Monographs of the Society for Research in Child Development, 50, 3-35. Bretherton, I. (1987). New perspectives on attachment relations: Security, communication, and internal working models. In: Osofoky (Ed.), Handbook of Infant Development (pp. 1061-1100). New York: Wiley. Brewer, W.F., & Nakamura, G.V. (1984). The nature and function of schemas. In: R.S. Wyer & T.X. Srull (Eds.), Handbook of social cognition. Hillsdale, NJ: Erlbaum. Bruner, J.S. ( 1964). The course of cognitive growth. American Psychologist, 19, 1-15. Burnham, D., Gladstonc, A., & Gibson, R. (1969). Schizophrenia and the Need-Fear Dilemma. New York: International Universities Press. Buss, D.M. (1987). Seletion, evocation, and manipulation. Journal of Personality and Social Psychology, 53, 1214-1221. Butter, S.R, & Strupp, H.H. (1986). Specific and nonspecific factors in psychotherapy: A problematic paradigm for psychotherapy research. Psychotherapy, 23, 30-40. Cantor, N. (1981). Perceptions of situations: Situation prototypes and person-situation prototypes. In: D. Magnusson (Ed.), Toward a psychology of situations: An interactional approach. Hillsdale, NJ: Erlbaum. Diamond, D. & Blatt, S.J. (1994). Internal working models of attachment and psychoanalytic theories of the representational world. A comparison and critique. In: M. Sperling & W.H. Bcrman (Eds.), Attachment in Adults: Theory: assessment, and treatment (pp. 72-97) New York: Guilford. Elicker, J., & Sroufc, L.A. (1992). Predicting peer competence and peer relationships in childhood from early parent-child relationships. In: R. Parke & A. Ladd (Eds.), Family-peer relationships: Modes of linkage (pp. 77-106). Hillsdale, NJ: Erlbaurn. Eikin, I., Shea, M.T., Watkins, J.T., Imber. S.D., Sotsky, S.M., Collins, J.F, Glass, D.R., Pilkonis, P., Leber, W.K., Dockerty, J.P., Fiester, S.J., & Parloff, M.B. (1989). NIMH Treatment of Depression Collaborative Research Program: General effectiveness of treatment. Archives of General Psychiatry, 46, 971-983. Emde, R.N. (1988). Development terminable and interminable. International Journal of Psycho-Analysis, 69, 23-42. Emde, R.N. (1983). The pre-representational self and its affective core. The Psychoanalytic Study of the Child, 38, 165-192. Erdelyi, M.A. (1985). Psychoanalysis: Freud's Cognitive Psychology. Oxford: Freeman. Erikson, E.H. (1950). Childhood and Society. New York: Norton. Erikson, E.H. (1968). Identity, Youth and Crisis. New York: Norton. Fantz, R.L. (1963). Pattern vision in newborn infants. Science, 140, 296-297. Fantz, R.L. (1966). Pattern discrimination and selective attention as determinants of perceptual development from birth. In: A.H. Kidd & J.L. Rivoire (Eds.), Perceptual development in children (pp. 143-173). New York: International Universities Press. Federn, P. (1952). Ego psychology and the psychoses. New York: Basic Books. Feffer, M. (1959). The cognitive implications of role-taking behavior. Journal of Personality, 27, 152-163. Feffer, M. (1970). Developmental analysis of interpersonal behavior. Psychology Review, 77, 177-214- Fiske, S.T., & Taylor, S.E. (1984). Social cognition. Reading, MA: Addison and Wesley. Fonagy, P., Steete, M., Moran, G., Steele, H., & Higgit, A. (199 1). Measuring the ghost in the nursery: A summary of the main findings of the Anna Freud Center-University College London Parent-Child Study. Bulletin of the Anna Freud Center, 14, 115-131. Fonagy, P., Steete, H., Steele, M. (1991). Maternal representations of attachment during pregnancy predict the organization of infant-mother attachment at one year of age. Child Development, 62, 891-905. Fraiberg, S. (1969). Libidinal object constancy and mental representation. Psychoanalytic Study of the Child, 24, 9-47. Fraiberg, S., Adelson, E., & Shapiro, V. (1975). Ghosts in the nursery: A psychoanalytic approach to impaired infant-mother relationships. Journal of the Academy of Child Psychiatry, 14, 387-421. Franz, C.E., & White, K.M. (1985). Individuation and attachment in personality development: Extending Erikson's theory. Journal of Personality, 53, 224-256. Freeman, T, Cameron, J.L., & McGhie, A. (1966). Studies on psychosis. New York: International Universities Press. Freud, S. (1929 [1930]). Civilization and its discontents. The standard edition of the complete psychological works of Sigmund Freud, 21, 64-145. London: Hogarth Press, 1957. Gardner, H. (1985). The mind's new science: A history of the cognitive revolution. New York: Basic Books. George, C. & Solomon, 1 (1989). Internal working models of care-giving and security of attachment at age six. Special issue: Internal representations and parent infant relationships. Infant Mental Health Journal, 10, 222-237. Gilligan, L. (1982). In a different voice: psychological theory and women's development. Cambridge, MA: Harvard University Press. Gilligan, C. (1989). Remapping the moral domain. In: C. Gilligan, V. Ward, & J.M. Taylor (Eds.), Mapping the moral domain (pp. 3-19). Cambridge, MA: Harvard University Press. Grossman, K, Fremmer-Bombik, E., Rudolph, J., Grossman, K.E.(1988). Maternal attachment representation as related to patterns of mother-infant attachment and maternal care during the first year. In: R.A. Hinde & J. Stevenson-Hinde (Eds.), Relationships within families: Mutual influences (pp. 241-260). Oxford: Clarendon Press. Gunderson, J.G. (1984). Borderline personality disorder. Washington, D.C.: American Psychiatric Press. Hastic, R. (1981). Schematic principles in human memory. In: E.T. Higgins, P. Herman, M.P. Zanna (Eds.), Social cognition: The Ontario Symposium, and Social Psychology (pp. 39-88). Hillsdale, NJ: Erlbaum. Hazan, C., & Shaver, P.R. (1990). Love and Work: An attachment-theoretical perspective. Journal of Personality and Social Psychology, 59, 270-280. Horowitz, M.J. (1972). Modes of representation of thought. Journal of the American Psychoanalytical Association, 20, 793-819. Hubel, D.H., & Wiesel, T.N. (1959). Receptive fields of single neurons in the cat's striate cortex. Journal of Physiology, 148, 574-591. Hubel, D.H., & Wiesel, T.N. (1962). Receptive fields, binocular interaction, and the functional architecture in the cats visual cortex. Journal of Physiology, 160, 106-154. Imber, S.D., Pilkonis, P.A., Sotsky, S.M., Elkin, I., Watkins, J.T, Collins, J.F., Shea, M.T, Leber, W.R., & Glass, D.R. (1990). Mode-specific effects among three Treatments for depression. Journal of Consulting and Clinical Psychology, 58, 352-359. Inhelder, B., & Piaget, J. (1959/1964). The early growth of logic in the child: classification of seriation. New York: Harper & Row (1964). Kelly, G.A. (1955). The psychology of personal constructs. New York: Norton. Kernberg, O.F. (1975). Borderline conditions and pathological narcissism. New York: Aronson. Kernberg, O.F. (1976). Object relations theory and clinical psychoanalysis. New York: Aronson. Kernberg, O.F. (1990). New perspectives in psychoanalytic affect theory. Emotion: Theory, Research and Experience, 5, 115-13 1. Kernberg, O.F. (1993). Psychoanalytic object relations theories. In: B.E. Moore and B. Fine (Eds.), Psychoanalysis: The major concepts. New Haven, CT: Yale University Press. Kihlstrom, J.E, & Cantor, N.C. (1984). Mental representations of the self. In: L. Berkowitz (Ed.), Advances in experimental social psychology, 17. New York: Academic Press. Kihlstrom, J.F, & Cunningham, R.L. (1991). Mapping interpersonal space. In: M.J. Horowitz (Ed.), Person schemas and maladaptive patterns (pp. 311-336). Chicago, IL: University of` Chicago Press. Klein, G.S. (1976). Psychoanalytic Theory: An exploration of essentials. New York: International Universities Press. Kobak, R., & Hazan, C. (1991). Attachment in marriage: Effects of security and accuracy of working models. Journal of Personality and Social Psychology, 60, 861-869. Kobak, R., & Sceery, A. (1988). Attachment in later adolescence: Working models affect regulation and representations of self and others. Child Development, 59, 135-146. Kohut, H. (1971). The analysis of the self. New York: International Universities Press. Kohut, H. (1977). The restoration of the self. New York: International Universities Press. Laurendeau, M., & Pinard, A. (1962). Casual Thinking in the Child: A genetic and Experimental Approach. New York: International Universities Press. Laurendeau, M., & Pinard, A. (1970). The Development of the Concept of Space in the Child. New York: International Universities Press. Levy, K.M., Blatt, S.J., & Shaver, P.R. (in press). Attachment style and mental representation in young adults. Journal of Personality & Social Psychology. Lichtenberg, J. (1985). Response: In search of the elusive baby. Psychoanalytic Inquiry, 5, 621-648. Lidz, R.W., & Lidz, T. (1952).Therapeutic considerations arising from the intense symbiotic nerds of schizophrenic patients. In: E.B. Brody & F.C. Redlich (Eds.), Psychotherapy with schizophrenics (pp. 168-178). New York: International Universities Press. Lidz, T. (1973). The origins of treatment of schizophrenic disorders. New York: Basic Books. Loewald, H. W. ( 1960). On the therapeutic action of psychoanalysis. International Journal of Psycho-Analysis, 41, 16-33. Loewald, H. W. (1962). Internalization, separation, mourning, and the superego. Psychoanalytic Quarterly, 31, 483-504. Lyons-Ruth, K. (1991). Rapprochement or rapprochement: Mahler's theory reconsidered from the vantage point of recent research on early attachment relationships. Psychoanalytic Psychology, 8, 1-24- Maddi, S. (1980). Personality theories: A comparative analysis (4th Edition). Homewood, IL: Dorsey. Mahler, M.S., Pine, E., & Bergman, A. (1975). The psychological birth of the human infant. New York: Basic Books. Main, M., Kaplan. N., & Cassidy J. (1985). In: I. Bretherton and E. Waters (Eds.), Growing points of attachment theory and research. Monograph of the Society for Research in Child Development, 50, 66-104. Main M. & Cassidy, J. (1988). Categories of response to reunion with the parent at age 6: Predicable from infant attachment classifications and stable over a 1 month period. Developmental Psychology, 24, 415-426. Mandler, J.M. (1988). How to build a baby: On the development of an accessible representational system. Cognitive Development, 3, 113-136. Marmor, J. (1953). Orality in the hysterical personality. Journal of the American Psychoanalytic Association, 1, 656-67 1. Masterson, J.G., & Rinsley, D.B. (1975). The borderline syndrome: The role of the mother in the genesis and psychic structure of the borderline personality. International Journal of Psycho-Analysis, 56, 163-177. Nelson, K. & Grundel, J. (1987). Generalized event representations: Basic building blocks of cognitive development. In: M. Lamb & A.L. Brown (Eds.), Advances in developmental psychology, Vol. 1 (pp. 131-158). Hillsdale, NJ: Lawrence Erlbaum Associates. Patterson, R.J. & Moran, G. (1988). Attachment Theory, personality development, and psychotherapy, Clinical Psychology Review, 8, 611-636. Piaget, J. (1937/1954). The construction of reality in the child (M. Cook, trans.). New York: Basic Books. Piaget, J. (1945/1962). Play, dreams and imitation in childhood. New York: Norton. Piaget, J. (1956). The origins of intelligence in the child (M. Cook, Trans.). New York: International Universities Press. Piaget, J. (1961/1969). The child's conception of time (A. J. Pomerans, Trans.). New York: Basic Books, 1961. Piaget, J., & Inhelder, B. (1969). The Psychology of the Child. New York: Basic Books. Ricks, M.H. (1985). The social transmission of parental behavior: Attachment versus generations. In: I. Bretherton & E. Waters (Eds.), Growing points of attachment theory and research. SCRD Monographs, 50 (6), 209. Rosenberg, S. (1988). Self and others: Studies in social psychology and autobiography. In: L. Berkowitz (Ed.), Advances in experimental social psychology, 21, 57-96. Orlando, FL: Academic. Rumelhart, D.E. (1980). Schemas: The building blocks of cognition. In: R. Spiro, B. Bracc, & W. Brewer (Eds.). Theoretical issues in reading comprehension (pp. 35-58). Hillsdale, NJ: Erlbaum. Sampson, E.E. (1985). Re-decentralization of identity: Toward a revised concept of personal and social order. American Psychologist, 40, 1203-1211. Sampson, E.E. (1988). The debate on individualism: Indigenous psychologies of the individual and their role in personal and societal functioning. American Psychologist, 43, 15-22. Sandier, J., & Rosenblatt, B. (1962). The concept of the representational world. The Psychoanalytic Study of the Child, 17, 128-145. Schaffer, C.E. (1993). "The rote of attachment in the experience and regulation of affect". Unpublishcd doctoral dissertation, Yale University, New Haven, Connecticut. Schank. R.C. & Abelson, R.P. (1977). Scripts, Plans, goals and understanding: An inquiry into human knowledge structures. Hillsdale, NJ: Lawrence Erlbaum. Searles, H.E (1965). Collected papers on schizophrenia and related subjects. New York: International Universities Press. Shakow, D. (1962). Segmental set: A theory of the formal psychological deficit in schizophrenia. Archives of General Psychiatry, 6, 1-17. Shaver, P. R., & Hazan, C. (1987). Being lonely, falling in love: Perspectives from attachment theory. Special Issue: Loneliness: Theory, research, and application. Journal of Social Behavior and Personality, 2, 105-124. Silverman, D.K. (1991). Attachment patterns and Freudian theory: An integration proposal. Psychoanalytic Psychology, 8, 169-193. Slade, A., & Aber. L.J. (1991). Attachment, drives and development: Conflicts and convergences in theory. In: J. Barron, M. Eagle, & D. Wolitzky (Eds.), Interface of Psychoanalysis and Psychology (pp. 154-185). Washington, D.C.: American Psychological Association. Sotsky, S.M., Glass, D.R., Shea, MT, Pilkonis, P.A., Collins, ].R., Elkin, I., Watkins, JT, Imber, S.D., Leber, W.R., Moyer J., & Oliveri, M.E. (1991). Patient predictors of response to psychotherapy and pharmacology: Findings of the NIMH Treatment of Depression Collaborative Research Program. American Journal of Psychiatry, 148, 997-1008. Sroufe, L.A. (1983). Infant-caregiver attachment and patterns of attachment in pre-school: The roots of matadaptive competence. In: M. Perlmutter (Ed.), Minnesota Symposium on child psychology, Volume 16 (pp. 41-83). Hillsdale, NJ: Lawrence Erlbaum Associates. Sroufc, L.A., Egeland, B., & Krcutzer, T. (1990). The fate of early experience following developmental change: Longitudinal approaches to individual adaptation in childhood. Child Development, 61, 1363-1373. Stern, D. N. (1985). The interpersonal world of the infant. New York: Basic Books. Surrey, J.L. (1985). The "self-in-relation": A theory of women's development. Work in Progress, 2. Wellesley, MA: Stone Center Working Papers. Tausk, V. (1919). On the Origin of the "Influencing Machine" in Schizophrenia. Psychoanalytic Quarterly, 1933, 2, 519-556. Taylor, S.E., & Crocker, J. (1981). Schematic bases of social information processing. In: E.T. Higgins, C.P. Herman, M.P. Zanna (Eds.), Social cognition: The Ontario Symposium on Personality and Social Psychology (pp. 89-134). Hillsdale, NJ.: Lawrence Erlbaum Associates. Wallerstein, R.S. (1986). Forty-two Lives in Treatment: A Study of Psychoanalysis and Psychotherapy. New York: Guilford. Werner, H. (1948/1957). Comparative Psychology of Mental Development. New York: International Universities Press. Werner, H., & Kaplan, B. (1963). Symbol formation: An organismic-developmental approach to language and the expression of thought. New York: Wiley. West, M. & Sheldon, A.E.R. (1988). Classification of pathological attachment patterns in adults. Journal of Personality Disorders, 2, 153.159. Witkin, A.H. (1965). Psychological Differentiation and Forms of Pathology. Journal of Abnormal Psychology, 70, 317-336. Witkin, A.H., Dyk, R.B., Faterson. H.I., Goodenough, D. R., & Karp, S. (1962). Psychological Differentiation. New York: Wiley. Zelnick, L., & Buchholtz, E. S. (1990). The concept of mental representations in light of recent infant research. Psychoanalytic Psychology, 7, 29-58. Zeanah, C.H., & Anders, T.F. (1987). Subjectivity in parent-infant relationships: A discussion of internal working models. Infant Mental Health Journal, 8, 237-250. Zeanah, C., Benoit, D., Hirshberg, L., Barton, M., & Regan, C. (1991). "Classifying mothers' representations of their infants: Results from structured interviews." Paper presented at the Annual Meeting of the American Academy of Child and Adolescent Psychiatry, San Francisco, CA. [Note: This paper appeared in: Dante Cicchetti & Sheree L. Toth, editors, Emotion, Cognition, and Representation (Rochester Symposium on Developmental Psychopathology, Volume 6). Rochester, NY: University of Rochester Press, 1995, pp. 1-33. We thank for the permission. The author is indebted to Kenneth M. Levy for his helpful comments on earlier drafts of this paper.]
Web Editor: Paolo Migone. For suggestions or corrections, please e-mail to: migone@unipr.it
|